📞Customer Service: +86 13248368268 📧servicecenter@suzhoufrank.com one year replacement and warranty!

Endoscopy Trainer vs Endoscopy Simulator: What's the Difference?
Compare endoscopy trainers and simulators for medical education. Understand costs, capabilities, and integration strategies for effective skill training.
MEDICAL TRAINING
Dr Qi Rui
3/8/20266 min read

Medical education programs often use the terms "endoscopy trainer" and "endoscopy simulator" interchangeably, leading to confusion among program directors, procurement teams, and trainees themselves. While both serve the goal of developing procedural competency, these training tools differ in design philosophy, functionality, and appropriate use cases within GI training curricula. Understanding these distinctions helps institutions select the right equipment for their educational objectives and budget constraints.
Defining the Endoscopy Trainer
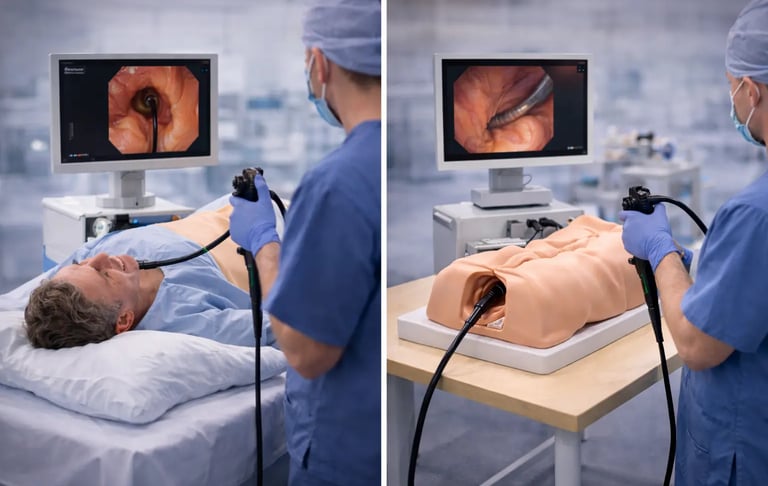
An endoscopy trainer refers primarily to physical, mechanical platforms designed to teach fundamental scope handling and navigation skills. These devices typically consist of anatomical phantoms constructed from silicone or similar soft materials, mounted within rigid external cases that replicate body cavities. The cavity allows insertion of a standard clinical endoscope, enabling trainees to practice basic maneuvers in a tangible, hands-on environment.
The key characteristic of an endoscopy trainer is its emphasis on tactile realism. Because trainees manipulate actual endoscopes through physical materials that approximate tissue resistance, mechanical trainers excel at teaching the foundational motor skills required for scope advancement, torque application, and dial control. Research published in Clinical Endoscopy notes that mechanical models offer advantages including lower cost compared to virtual alternatives, effectiveness during initial training phases, and superior haptic realism compared to computer-based systems.
Common examples of endoscopy trainers include box trainers with interchangeable modules for practicing specific tasks such as retroflexion, loop reduction, or polypectomy targeting. These platforms work well for deconstructed skill practice where trainees focus on individual competencies before integrating them into complete procedures. For GI training programs seeking cost-effective solutions for early-stage education, physical trainers represent an accessible entry point.
Suzhou Frank supplies several physical training models suited to this category. The Gastrointestinal Endoscopy Simulator provides realistic upper GI tract anatomy for practicing diagnostic EGD maneuvers, while the Bronchoscopy Simulator Type A and Type B models offer respiratory tract training with four-level bronchial branch configurations compatible with commercial fiberoptic bronchoscopes.
Understanding the Endoscopy Simulator
An endoscopy simulator encompasses a broader category that includes computerized virtual reality systems, hybrid platforms combining physical and digital elements, and sophisticated mechatronic devices providing electronic feedback. These systems aim to create comprehensive training environments that address not only technical skills but also cognitive competencies such as lesion recognition, adverse event management, and clinical decision-making.
Virtual reality simulators represent the most technologically advanced end of this spectrum. These platforms use sensor-equipped scope interfaces connected to computer systems that generate real-time visual feedback on monitors. As trainees manipulate the instrument, the virtual environment responds with corresponding changes in endoscopic imagery, patient comfort indicators, and procedure metrics. A comprehensive review in Cancers journal explains that computerized simulators offer significant advantages including the ability to simulate multiple procedures on a single platform, reproducible training scenarios across all trainees, and objective measurement matrices for competency assessment.
The distinguishing feature of advanced simulators lies in their capacity for standardization and data collection. Training directors can ensure every trainee experiences identical case complexity, enabling fair comparisons of performance and systematic tracking of learning curves. Many systems provide immediate feedback on metrics such as time to reach anatomical landmarks, percentage of mucosa visualized, and patient discomfort levels simulated through audio-visual cues.
However, simulators carry higher acquisition and maintenance costs. Virtual reality platforms can range from tens of thousands to over one hundred thousand dollars, placing them beyond reach for many smaller training programs. Additionally, despite technological advances, haptic feedback in computerized systems often falls short of the tactile realism provided by physical trainers or animal models.
Key Differences Between Trainers and Simulators
The practical distinctions between these training tools emerge across several dimensions that affect purchasing decisions and curriculum integration. Training program directors must evaluate these differences carefully when allocating limited educational budgets and designing curricula that prepare trainees for independent practice.
Physical portability represents an often-overlooked consideration. Many endoscopy trainers feature compact, lightweight designs that allow transport between training sites or storage when not in active use. This flexibility enables satellite training at affiliated hospitals or community clinics without requiring permanent simulation laboratory space. Virtual simulators typically require dedicated installation with stable positioning for their mechanical feedback systems, limiting mobility between locations.
Regarding cost and accessibility, endoscopy trainers typically range from several hundred to a few thousand dollars, making them feasible for institutions with limited budgets or those establishing new training programs. Simulators, particularly VR-based systems, require substantially larger capital investments plus ongoing software licensing and maintenance expenses. For programs in the early stages of simulation curriculum development, physical trainers often serve as foundational equipment while funding is secured for more advanced systems.
In terms of skill focus, trainers excel at teaching isolated motor skills through repetitive practice of specific maneuvers. Trainees can spend concentrated time mastering scope handling before facing the cognitive demands of lesion identification or therapeutic intervention. Simulators better support integrated skill development where trainees must simultaneously manage technical execution, visual interpretation, and clinical reasoning within realistic case scenarios.
Feedback mechanisms differ substantially between categories. Physical trainers provide natural tactile feedback through material properties but offer no objective performance measurement unless supplemented with external evaluation tools. Computerized simulators automatically capture extensive procedural data, enabling quantitative assessment of competency progression. For programs implementing skills assessment protocols, this data collection capability proves valuable for documentation and credentialing purposes.
Scenario versatility represents another differentiator. A given physical trainer typically addresses one anatomical region or procedure type, requiring multiple devices to cover comprehensive training needs. Virtual simulators can house extensive case libraries spanning upper GI, lower GI, ERCP, and therapeutic procedures within a single platform, though each module may require separate licensing fees.
When to Use Each Type of Training Tool
Effective training programs typically employ both trainers and simulators at appropriate stages of learner development rather than relying exclusively on either approach. The medical simulation guide provides comprehensive frameworks for integrating various training modalities.
For complete beginners with no prior endoscopy experience, starting on physical trainers allows focus on fundamental scope mechanics without overwhelming cognitive load. Trainees can develop muscle memory for dial manipulation, insertion tube rotation, and coordinated advancement before encountering clinical scenarios requiring diagnostic interpretation. Models like the Gastrointestinal ESD Surgical Simulator enable progressive skill building from basic navigation through advanced therapeutic techniques.
As trainees demonstrate proficiency in basic handling, transitioning to simulator-based cases introduces realistic clinical complexity. Virtual environments challenge learners to apply their technical skills while managing patient comfort, identifying pathology, and making procedural decisions. This progression mirrors the educational philosophy of simulation-based mastery learning, where trainees must demonstrate competency at each level before advancing.
For therapeutic procedure training, hybrid approaches often prove most effective. Physical or ex-vivo models provide superior haptic realism for learning tissue interaction during techniques such as polypectomy, hemostasis, or dissection. Virtual simulators complement this by allowing extensive case volume exposure and scenario variation without consumable costs associated with biological specimens.
Programs focused on competency training benefit from combining both modalities strategically throughout fellowship curricula rather than viewing them as competing alternatives.
Expanding Training Across Specialties
While GI endoscopy drives much of the training equipment market, the principles distinguishing trainers from simulators apply across endoscopic specialties. Programs training fellows in pulmonology, urology, or gynecology face similar equipment selection decisions.
The Ultrasound Bronchoscopy Simulator addresses pulmonary training needs with endobronchial ultrasound capabilities increasingly important for lung cancer staging. Urological programs can utilize the Urological Endoscopy Simulator for cystoscopy and related procedure training. The Hysteroscopy Simulator provides gynecologic endoscopy training with realistic uterine anatomy.
Cross-specialty exposure within larger medical centers allows efficient equipment utilization, with scheduling systems enabling multiple departments to share simulation resources. This approach maximizes return on equipment investments while exposing trainees to procedural parallels across endoscopic disciplines.
About Suzhou Frank Medical
Suzhou Frank Intelligent Technology Co., Ltd., headquartered in Suzhou, Jiangsu Province, China, specializes in medical endoscopic imaging systems and clinical simulation training equipment. The company develops HD and fluorescence imaging systems, 3D/4K endoscopy platforms, and comprehensive training simulators that support standardized medical education across endoscopic specialties.
With commitment to quality manufacturing and responsive technical support, Suzhou Frank serves medical institutions establishing or expanding simulation-based training programs. The company's complete product catalog includes trainers and simulators spanning gastrointestinal, respiratory, urological, and gynecologic applications. Program directors and procurement teams can contact Suzhou Frank directly to discuss equipment specifications, pricing, and institutional needs assessment.
Conclusion
The distinction between endoscopy trainers and simulators reflects differences in technology, cost, and pedagogical application rather than quality or effectiveness. Physical trainers provide accessible, tactile-focused platforms ideal for foundational skill acquisition. Computerized simulators offer comprehensive training environments with objective measurement capabilities suited to integrated competency development and assessment. Most successful training programs employ both approaches strategically, matching equipment selection to learner stage and educational objectives. Understanding these distinctions enables informed equipment decisions that align with institutional resources and curricular goals.
© 2025. All rights reserved.
About Us
Introduction
Development
Cooperation
Service
Main Products
Medical Grade Monitor
No 15, Jinyang road KunshanSuzhou, Jiangsu, China